If you work in an ED, you know what a "frequent flier" is. It is a patient that visits on a regular basis and unfortunately, usually one that you are not happy to see. I can remember a number of them that we have had in our department over the years. One was a 40-ish female smoker and drug user with severe asthma who came in several times weekly sitting straight up on the ambulance stretcher, grasping the nebulizer mask with that panicked look of someone who can't breathe. She had very poor veinous access and on several occasions, an IO had to be performed (a catheter straight into the bone). We would stabilize her breathing and she would go outside to wait for a ride… and smoke. On several of her visits she begged to be intubated due to the severity of the attack and she a few times she actually was. On her last visit, she never made it off the ventilator.
Another woman I remember was also in her 40’s, was a bilateral amputee, and a prostitute. She looked pretty worn, and definitely not the part of a lady of the evening, but from what I hear, she had been beautiful. Her disease had been peripheral vascular disease, causing her to lose both legs and have multiple infections. She would make her rounds of the different hospitals and ER’s looking for pain medicines and antibiotics. She has passed as well.
Most of the frequent fliers that we see currently are our intoxicated residents, usually homeless men. They are picked up by the police for passing out in the wrong public place or making a disturbance. Their blood alcohol levels are probably 150-200 as an average, and the ER is not supposed to let an intoxicated individual leave until they are under 100. There lies the dilemma. The protocol is that they should also have a sober individual to accompany them. We groan when we see them because they are almost always reeking of alcohol, sweat, vomit, and other unmentionable things. They curse, swing their fists and demand things. We give them some IV fluids, and if they are relatively stable, send them back on their way. One man fell during a drunken evening and broke his jaw, necessitating his jaw being wired shut. He could still drink alcohol through a straw. The next time we saw him, he had fallen backwards and broken a cervical vertebrae.
Yesterday, I was the lucky recipient of one of our fliers, one who has been in our department 4 times in 3 days. He is a long term alcoholic and heroin user and claims to have lost everything. He had a large mason tool in his belonging which we discreetly moved so it wouldn’t become a hurled missile. When asked why he was back this time, he said, “I think I have heat stroke”. It is very hot if Florida and he had been wandering around but I saw no cramping or classic signs of heat stroke. The day before he had been to the ER twice, the second time because he had fallen right outside our department. I tried to contain my frustration, as we were quite busy, but as he rambled on, I really had had enough when he said, “I really just want attention”. I promptly left to go take care of my dialysis patient with the distended abdomen.
I was less than friendly to him and did not pay him much attention. The doctors are not patient with these folks and we do little to help them. We also can't watch them constantly and can't force them to stay. When I returned to the room he was gone and when I left for the day 30 minutes later, he was standing on the sidewalk, aimlessly walking up and down. I pretended I didn’t see him and hurried to my car. But I must admit I felt a bit ashamed. Could I have done something more? I feel that I have helped thousands of people in the almost 20 years of nursing I have done. But the ones I haven’t helped are the ones that stick out.

Sunday, August 1, 2010
Sunday, July 25, 2010
Ask an ER Nurse!
In the emergency room we frequently get “nurse calls” which are local residents calling the ER with a medical question they would like an answer to. The ER secretary will either send the question to the charge nurse, the triage nurse, or will overhead page “Nurse call on line 431”. What are these folks calling to ask about? You name it, all kinds of things.
Many calls involve a prior visit to the ER and the patient now has questions or worsening symptoms. The nurse taking the call can usually answer a general question or may have to go into the computer to look up the record to see what the ER physician had in mind for treatment. If the patient is not improving or wants a different medication, they mistakenly think we can fix that for them over the phone. When we tell them they would have to come in for a new visit, they must think we are just out for more business. There is no way that we can change prescriptions over the phone or even verify who is calling. Often times, the doctor who treated the patient is not on duty. If the patient comes in to the ER with a legitimate problem, like a reaction to an antibiotic, I have seen a physician write a new prescription without making the individual sign back in.
Some calls to the ER are to give a list of symptoms and get the opinion of the nurse as to whether an ER visit is necessary. I try to stop myself from saying, “hold the arm with the rash up to the phone and I’ll let you know”! Seriously, we try to listen for warning signs like swollen tongues, trouble breathing, lips that are turning blue, or someone who isn’t responding appropriately. We will advise the caller to dial 911 if we think it sound serious enough and we don’t want the patient driven here. I actually had a lady call and tell me that her mother was slumped over in the chair, non-responsive and drooling and wondered what to do. I calmly told her to hang up and dial 911. I hope she did.
I have 20 years of nursing experience and I thought it would be interesting to see if I could get blog traffic to pose questions for me to answer and share. Questions regarding medications, aggravating symptoms, what type of doctor to go to, why we do what we do in the ER, that kind of thing. Please post a comment to this blog with a question and I will answer it within a day!
Let me state the necessary disclaimer that I am giving nursing advice, not medical opinion, and I am in no way bound or responsible for what the individual posing the question does with that information. If you post to my blog, you are consenting to this disclaimer. Thank you very much!!!
Many calls involve a prior visit to the ER and the patient now has questions or worsening symptoms. The nurse taking the call can usually answer a general question or may have to go into the computer to look up the record to see what the ER physician had in mind for treatment. If the patient is not improving or wants a different medication, they mistakenly think we can fix that for them over the phone. When we tell them they would have to come in for a new visit, they must think we are just out for more business. There is no way that we can change prescriptions over the phone or even verify who is calling. Often times, the doctor who treated the patient is not on duty. If the patient comes in to the ER with a legitimate problem, like a reaction to an antibiotic, I have seen a physician write a new prescription without making the individual sign back in.
Some calls to the ER are to give a list of symptoms and get the opinion of the nurse as to whether an ER visit is necessary. I try to stop myself from saying, “hold the arm with the rash up to the phone and I’ll let you know”! Seriously, we try to listen for warning signs like swollen tongues, trouble breathing, lips that are turning blue, or someone who isn’t responding appropriately. We will advise the caller to dial 911 if we think it sound serious enough and we don’t want the patient driven here. I actually had a lady call and tell me that her mother was slumped over in the chair, non-responsive and drooling and wondered what to do. I calmly told her to hang up and dial 911. I hope she did.
I have 20 years of nursing experience and I thought it would be interesting to see if I could get blog traffic to pose questions for me to answer and share. Questions regarding medications, aggravating symptoms, what type of doctor to go to, why we do what we do in the ER, that kind of thing. Please post a comment to this blog with a question and I will answer it within a day!
Let me state the necessary disclaimer that I am giving nursing advice, not medical opinion, and I am in no way bound or responsible for what the individual posing the question does with that information. If you post to my blog, you are consenting to this disclaimer. Thank you very much!!!
Friday, July 16, 2010
Who is at Risk for a Spontaneous Pneumothorax?
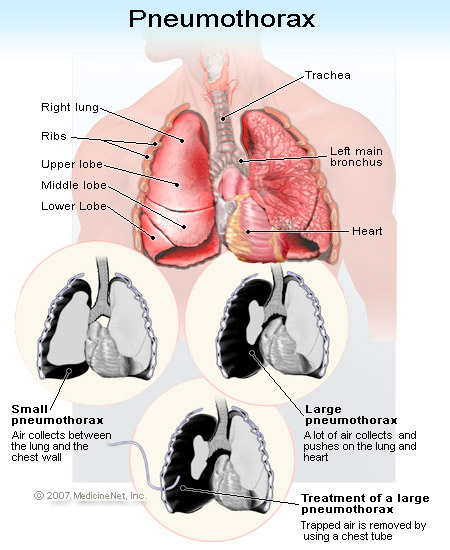
A pneumothorax or, “collapsed lung”, is often first seen and diagnosed in the Emergency Department. Identifying the condition in triage is crucial so as to prevent hypoxia (inadequate oxygen reaching the tissues). An experienced nurse may recognize this condition best by the characteristics of the individual: a male between the ages of 20 and 40, particularly tall and thin, and a smoker. He may present with sudden onset of chest pain, sharp in nature with feelings of tightness in the chest. Shortness of breath, rapid heart rate, rapid breathing, cough, and fatigue are other symptoms. If the skin has developed a bluish color (termed cyanosis), haste in treatment is vital.
So what is a pneumothorax? A pneumothorax is a collection of free air in the chest outside the lung that causes the lung to collapse. A spontaneous pneumothorax, also referred to as a primary pneumothorax, occurs in the absence of a traumatic injury to the chest or a known lung disease. It is caused by a rupture of a cyst or a small sac (bleb) on the surface of the lung. Pneumothorax may also occur following an injury to the chest wall such as a fractured rib, any penetrating injury (gun shot or stabbing), surgical invasion of the chest, or may be deliberately induced in order to collapse the lung. A pneumothorax can also develop as a result of underlying lung diseases, including cystic fibrosis, chronic obstructive pulmonary disease (COPD), lung cancer, asthma, and infections of the lungs.
Spontaneous pneumothorax affects about 9,000 persons each year in the U.S. who have no history of lung disease. Smoking has been shown to increase the risk for spontaneous pneumothorax.
To verify diagnosis, examination of the chest with a stethoscope reveals decreased or absent breath sounds over the affected lung. The diagnosis is confirmed by chest x-ray.
A small pneumothorax without underlying lung disease may resolve on its own in one to two weeks. A larger pneumothorax and a pneumothorax associated with underlying lung disease often require aspiration of the free air and/or placement of a chest tube to evacuate the air. Possible complications of chest tube insertion include pain, infection of the space between the lung and chest wall (the pleural space), hemorrhage (bleeding), fluid accumulation in the lung, and low blood pressure (hypotension). In some cases, the leak does not close on its own. This is called a bronchopleural fistula, and may require chest surgery to repair the hole in the lung.
The outcome of a pneumothorax depends upon the extent and type of pneumothorax. A small spontaneous pneumothorax will generally resolve on its own without treatment. A secondary pneumothorax associated with underlying disease, even when small, is much more serious and carries a 15% mortality rate. A secondary pneumothorax requires urgent and immediate treatment. Having one pneumothorax increases the risk of developing the condition again. The recurrence rate for both primary and secondary pneumothorax is about 40%; most recurrences occur within 1.5 to two years.
The nurse’s role in the ED is vital in identification upon presentation and in carrying out treatment. The patient will be understandably anxious, scared and uncomfortable. Education and reassurance needs to be given to both the patient and family members. The ED physician will need assistance if a chest tube is to be inserted and preparation includes obtaining consent, set up of the equipment, and pre-medications and monitoring of vital signs/oxygenation. The patient will most times be admitted and will need follow up care. Try to bite your tongue on the smoking cessation lecture (if warranted) until the patient is once again comfortable!

Medical Revising Authors and Editor: George Schiffman, MD, and Melissa Conrad Stoppler, MD
So what is a pneumothorax? A pneumothorax is a collection of free air in the chest outside the lung that causes the lung to collapse. A spontaneous pneumothorax, also referred to as a primary pneumothorax, occurs in the absence of a traumatic injury to the chest or a known lung disease. It is caused by a rupture of a cyst or a small sac (bleb) on the surface of the lung. Pneumothorax may also occur following an injury to the chest wall such as a fractured rib, any penetrating injury (gun shot or stabbing), surgical invasion of the chest, or may be deliberately induced in order to collapse the lung. A pneumothorax can also develop as a result of underlying lung diseases, including cystic fibrosis, chronic obstructive pulmonary disease (COPD), lung cancer, asthma, and infections of the lungs.
Spontaneous pneumothorax affects about 9,000 persons each year in the U.S. who have no history of lung disease. Smoking has been shown to increase the risk for spontaneous pneumothorax.
To verify diagnosis, examination of the chest with a stethoscope reveals decreased or absent breath sounds over the affected lung. The diagnosis is confirmed by chest x-ray.
A small pneumothorax without underlying lung disease may resolve on its own in one to two weeks. A larger pneumothorax and a pneumothorax associated with underlying lung disease often require aspiration of the free air and/or placement of a chest tube to evacuate the air. Possible complications of chest tube insertion include pain, infection of the space between the lung and chest wall (the pleural space), hemorrhage (bleeding), fluid accumulation in the lung, and low blood pressure (hypotension). In some cases, the leak does not close on its own. This is called a bronchopleural fistula, and may require chest surgery to repair the hole in the lung.
The outcome of a pneumothorax depends upon the extent and type of pneumothorax. A small spontaneous pneumothorax will generally resolve on its own without treatment. A secondary pneumothorax associated with underlying disease, even when small, is much more serious and carries a 15% mortality rate. A secondary pneumothorax requires urgent and immediate treatment. Having one pneumothorax increases the risk of developing the condition again. The recurrence rate for both primary and secondary pneumothorax is about 40%; most recurrences occur within 1.5 to two years.
The nurse’s role in the ED is vital in identification upon presentation and in carrying out treatment. The patient will be understandably anxious, scared and uncomfortable. Education and reassurance needs to be given to both the patient and family members. The ED physician will need assistance if a chest tube is to be inserted and preparation includes obtaining consent, set up of the equipment, and pre-medications and monitoring of vital signs/oxygenation. The patient will most times be admitted and will need follow up care. Try to bite your tongue on the smoking cessation lecture (if warranted) until the patient is once again comfortable!
Medical Revising Authors and Editor: George Schiffman, MD, and Melissa Conrad Stoppler, MD
Sunday, July 11, 2010
I Feel Good....Didn't Know That I Would!
How we feel and how we live our life is I think about 90% attitude and health and 10% circumstance. It sounds cliché to say "stay positive", but a positive mental attitude is everything! Anything that happens to you or those around you can be effectively handled if you can look at it from a positive perspective. We all can name specific individuals in our lives that we tend to avoid because everything that comes out of their mouths is doom and gloom. You can almost see the sneer on their face!
Being healthy is the other logical part of living well. Americans are horrible at this. Drive thru's, take out, junk food everywhere and super-sizes combined with video games and remote controls = obesity. I personally do not have a weight problem, but I know I would feel better with 20 less pounds and would be at a perfect size for my height if I could get there. I've had problems with migraines for years and a neurologist recently told me to first try giving up caffeine. Being a nurse, I of course know that caffeine is not good for you, but it's been my only vice besides chocolate. I drank 2 cups of coffee and 2 Diet Coke's a day. But after increasing headaches drove me to the neurologist, it took his advice to get me to quit. I have now given up the Diet Cokes and am down to 1 cup of half-caffeine coffee a day. And guess what, this morning I noticed that I really do feel energized! I did a work out with weights with more vigor than before and am mentally ready to tackle tasks I usually am sluggish to do!
Whether we are nurses, doctors, or rocket scientists, we all know what is good for us... but actually putting it into play is different. Personal change is SO hard! But when you can accomplish it, the feeling of satisfaction is amazing. My next step is to cut my food intake almost in half. I want to prepare my family's dinner plates like usual, and then take almost half my food and put it away for another meal. This will save money too! No snacking and lots of water.
Life is a work in progress.....
Being healthy is the other logical part of living well. Americans are horrible at this. Drive thru's, take out, junk food everywhere and super-sizes combined with video games and remote controls = obesity. I personally do not have a weight problem, but I know I would feel better with 20 less pounds and would be at a perfect size for my height if I could get there. I've had problems with migraines for years and a neurologist recently told me to first try giving up caffeine. Being a nurse, I of course know that caffeine is not good for you, but it's been my only vice besides chocolate. I drank 2 cups of coffee and 2 Diet Coke's a day. But after increasing headaches drove me to the neurologist, it took his advice to get me to quit. I have now given up the Diet Cokes and am down to 1 cup of half-caffeine coffee a day. And guess what, this morning I noticed that I really do feel energized! I did a work out with weights with more vigor than before and am mentally ready to tackle tasks I usually am sluggish to do!
Whether we are nurses, doctors, or rocket scientists, we all know what is good for us... but actually putting it into play is different. Personal change is SO hard! But when you can accomplish it, the feeling of satisfaction is amazing. My next step is to cut my food intake almost in half. I want to prepare my family's dinner plates like usual, and then take almost half my food and put it away for another meal. This will save money too! No snacking and lots of water.
Life is a work in progress.....
Monday, June 7, 2010
Triage - why did she get called first!
The word triage comes from the French word trier, which means "to sort". During a mass casualty or disaster, triage is used to determine how time and resources should be used. If a person is found with no breathing or heartbeat, he would be given the classification "E" - expectant, and sadly, left to die. A victim with massive bleeding and spontaneous breathing wound be classified as "I", immediate, whose life could be saved if given prompt treatment. A victim with an obvious broken arm but no bleeding and no breathing difficulties would be given a "D", delayed, an obvious meaning. The walking wounded - scrapes and bruises would be "M" - minimal and could wait indefinitely.
In day-to-day life, in the absence of disaster, triage is used in the emergency department to decide who will see the doctor first. My hospital, like many, uses a 5 tiered system. "5" is given to a patient coming in for suture removal or the recheck of a wound. A patient with a sore throat or cold would be given a "4" and could wait a long time with no harm done. The person with nausea and vomiting, abdominal pain, or a broken arm wound be given a "3" which means they need to be treated as soon as possible, but there is no imminent danger to their life or limb. The man who comes in looking pale, sweating, and clutching his chest, complaining of chest pain would be given a "2" - needing of immediate treatment or there could be a threat to life. We reserve the rating of "1" for the patient that EMS brings in with CPR in progress or a person with stroke symptoms prior to complete unresponsiveness.
Working as a triage nurse can be a stressful position. In my department, certain nurses are routinely placed in triage for the day while most of the staff do direct patient care. The charge nurse relies on the triage nurse to keep things moving and to alert her when a patient has arrived who needs an immediate exam room open, but who won't bother her with multiple questions or updates. During a busy day, the triage nurse is also responsible for the patients in the waiting room who may be there for hours. The lady who comes in with abdominal pain may seem stable, but an hour later could become diaphoretic and pale with a decreased level of consciousness due to a rupturing aneurysm. That is the responsibility of the triage nurse to monitor. This can be overwhelming with 15-20 people waiting. Then there is dealing with the angry glares and multiple trips to the front desk from the man with the sore throat who sees the patients with chest pain and trouble breathing going first. The average citizen does not understand triage and assume they will get in to see the doctor in a similar fashion that they would get a table at the Outback.
The addition of urgent care centers has greatly reduced the number of patients coming in for minor ailments, but with the current health care crisis, many still rely on the ER for their needs because they have no insurance and cannot pay the up-front cost of an urgent care. So next time you find yourself waiting in the ER, even if you're uncomfortable, give the triage nurse some credit that she is not ignoring you or playing favorites when she wheels the semi-conscious patient into the back who came in after you did.
In day-to-day life, in the absence of disaster, triage is used in the emergency department to decide who will see the doctor first. My hospital, like many, uses a 5 tiered system. "5" is given to a patient coming in for suture removal or the recheck of a wound. A patient with a sore throat or cold would be given a "4" and could wait a long time with no harm done. The person with nausea and vomiting, abdominal pain, or a broken arm wound be given a "3" which means they need to be treated as soon as possible, but there is no imminent danger to their life or limb. The man who comes in looking pale, sweating, and clutching his chest, complaining of chest pain would be given a "2" - needing of immediate treatment or there could be a threat to life. We reserve the rating of "1" for the patient that EMS brings in with CPR in progress or a person with stroke symptoms prior to complete unresponsiveness.
Working as a triage nurse can be a stressful position. In my department, certain nurses are routinely placed in triage for the day while most of the staff do direct patient care. The charge nurse relies on the triage nurse to keep things moving and to alert her when a patient has arrived who needs an immediate exam room open, but who won't bother her with multiple questions or updates. During a busy day, the triage nurse is also responsible for the patients in the waiting room who may be there for hours. The lady who comes in with abdominal pain may seem stable, but an hour later could become diaphoretic and pale with a decreased level of consciousness due to a rupturing aneurysm. That is the responsibility of the triage nurse to monitor. This can be overwhelming with 15-20 people waiting. Then there is dealing with the angry glares and multiple trips to the front desk from the man with the sore throat who sees the patients with chest pain and trouble breathing going first. The average citizen does not understand triage and assume they will get in to see the doctor in a similar fashion that they would get a table at the Outback.
The addition of urgent care centers has greatly reduced the number of patients coming in for minor ailments, but with the current health care crisis, many still rely on the ER for their needs because they have no insurance and cannot pay the up-front cost of an urgent care. So next time you find yourself waiting in the ER, even if you're uncomfortable, give the triage nurse some credit that she is not ignoring you or playing favorites when she wheels the semi-conscious patient into the back who came in after you did.
Sunday, May 30, 2010
Putting a Face on Trauma
Are you more likely to be involved in a traumatic event this year? Studies have been done to tell us who is most likely to be brought in our ED doors on a stretcher. Trauma is defined as injury to human tissues and organs resulting from the transfer of energy from the environment. The term "accident" is being taken out of the current vocabulary since most traumatic injuries and deaths are preventable and don't happen by chance. Hence, the now accepted term for vehicle mayhem is "motor vehicle crash" instead of "motor vehicle accident".
Annually, approximately 164,112 deaths are the result of trauma. Those that survive enter the healthcare system with often long term needs and disabilities with loss of limb, deformity, and a decreased ability to earn a living. Adults between the ages of 35 and 44 are more like to die from being involved in some sort of traumatic event. The leading cause of death for every age group from the ages of 5 to 24 years is a motor vehicle crash (MVC). As far as gender goes, a male is 2.3 times more likely to be involved in injury-producing events than a female. Race also plays a part. A leading cause of death for Caucasians is MVC's. African Americans are most highly affected by intentional trauma between the ages of 10 and 24. Intentional traumas are usually gunshots, stabbings and other forms of assault. Hispanics have the highest rate of fatalities in work related injures, in part because of the agricultural and industrial type labor jobs they hold.
Not surprisingly, alcohol plays a role in almost all types of traumatic injury. The use of alcohol influences judgment, coordination, reflexes, balance and cognitive functions. With MVC deaths, studies have shown that 25% of drivers aged 15 to 20 years of age had a blood alcohol concentration of 0.08 g/dl or higher. Alcohol is also involved in 25-50% of adolescent and adult fatalities associated with water recreation.
Homicide is the leading cause of death among people aged 10 to 24 years. The increased availability of firearms contributes to the number of deaths from gunshots. Firearms are involved in approximately 70% of homicides, 60% of suicides, 40% of robberies, and 20% of aggravated assaults. Another intentional trauma is child mistreatment. It is estimated that between 1 and 3 million children per year are victims of intentional trauma.
Injury prevention is key in avoiding trauma and committees and researches work daily to enhance injury surveillance systems, develop firearm policies, and fund trauma care system development. Education of the public as well as our health-care providers is crucial to successfully intervene when trauma occurs.
Source: Trauma Nursing Core Course (TNCC) Provider Manual, Sixth Edition, Copyright 2007 by the Emergency Nurses Association.
Annually, approximately 164,112 deaths are the result of trauma. Those that survive enter the healthcare system with often long term needs and disabilities with loss of limb, deformity, and a decreased ability to earn a living. Adults between the ages of 35 and 44 are more like to die from being involved in some sort of traumatic event. The leading cause of death for every age group from the ages of 5 to 24 years is a motor vehicle crash (MVC). As far as gender goes, a male is 2.3 times more likely to be involved in injury-producing events than a female. Race also plays a part. A leading cause of death for Caucasians is MVC's. African Americans are most highly affected by intentional trauma between the ages of 10 and 24. Intentional traumas are usually gunshots, stabbings and other forms of assault. Hispanics have the highest rate of fatalities in work related injures, in part because of the agricultural and industrial type labor jobs they hold.
Not surprisingly, alcohol plays a role in almost all types of traumatic injury. The use of alcohol influences judgment, coordination, reflexes, balance and cognitive functions. With MVC deaths, studies have shown that 25% of drivers aged 15 to 20 years of age had a blood alcohol concentration of 0.08 g/dl or higher. Alcohol is also involved in 25-50% of adolescent and adult fatalities associated with water recreation.
Homicide is the leading cause of death among people aged 10 to 24 years. The increased availability of firearms contributes to the number of deaths from gunshots. Firearms are involved in approximately 70% of homicides, 60% of suicides, 40% of robberies, and 20% of aggravated assaults. Another intentional trauma is child mistreatment. It is estimated that between 1 and 3 million children per year are victims of intentional trauma.
Injury prevention is key in avoiding trauma and committees and researches work daily to enhance injury surveillance systems, develop firearm policies, and fund trauma care system development. Education of the public as well as our health-care providers is crucial to successfully intervene when trauma occurs.
Source: Trauma Nursing Core Course (TNCC) Provider Manual, Sixth Edition, Copyright 2007 by the Emergency Nurses Association.
Wednesday, May 26, 2010
Trauma! Give me an "A"!!
Last week I successfully completed the TNCC course which I first took in 2001 or 2002. TNCC is Trauma Nursing Core Course and it is sponsored by the Emergency Nurses Association. It is a national certification valid for 4 years. Whether or not we work in a trauma center, every emergency room has the potential to receive a trauma patient, sometimes because of inclement weather and the inability to get a helicopter in the air, sometimes because it happens in such close proximity that they are rolled in your door. The principle behind TNCC is to give the nurse a systematic approach to each patient, whether it is a victim of a car crash, an electrocution, drowning, or violent crime. Each patient should be approached in exactly the same manner and if all steps are followed, a positive outcome should ensue.
In a perfect world. It is not that difficult to memorize the steps and listen to a lecture with gruesome slides in a quiet, private classroom. A 50 question test is given at the end of the 2 days and a practical exam must be done one-on-one with an instructor. No step can be left out or the candidate fails. I am a good test taker and am not cursed with test anxiety like so many are, so the course went well for me.
But do you ever have a "normal" trauma, an organized situation where what I've learned can be done step by step? No, it is usually chaos with blood and fluids spraying, doctors yelling orders, and family members screaming. This also means that there are other members of a team that can help this patient, it is never really up to just one trauma nurse going through her steps as in TNCC.
I have been a nurse for 19 years, in the ER for 10, but I know I will assess my next trauma patient with new eyes. One of my favorite points that our instructor brought up:
A man comes in with a traumatic amputation of the lower leg. Everyone is trying to stop the bleeding, see if the amputated part was brought in, etcetera. But does the patient have a patent airway and is he breathing? Imagine applying a great pressure dressing and wrapping the severed part correctly only to find that the patient had vomited and aspirated, then asphyxiated while everyone was running about! It reminded me that no matter what horrible development has gone on with a trauma patient's body, none of it matters if you don't have an airway.
So the absolute main point of TNCC and its training is the most basic of principles which hails back to basic life support. A B C!!! Always airway and breathing, even before pulse, since once again, a pulse won't last long if there is no breathing involved.
More nuggets from this wonderful course on another day.
In a perfect world. It is not that difficult to memorize the steps and listen to a lecture with gruesome slides in a quiet, private classroom. A 50 question test is given at the end of the 2 days and a practical exam must be done one-on-one with an instructor. No step can be left out or the candidate fails. I am a good test taker and am not cursed with test anxiety like so many are, so the course went well for me.
But do you ever have a "normal" trauma, an organized situation where what I've learned can be done step by step? No, it is usually chaos with blood and fluids spraying, doctors yelling orders, and family members screaming. This also means that there are other members of a team that can help this patient, it is never really up to just one trauma nurse going through her steps as in TNCC.
I have been a nurse for 19 years, in the ER for 10, but I know I will assess my next trauma patient with new eyes. One of my favorite points that our instructor brought up:
A man comes in with a traumatic amputation of the lower leg. Everyone is trying to stop the bleeding, see if the amputated part was brought in, etcetera. But does the patient have a patent airway and is he breathing? Imagine applying a great pressure dressing and wrapping the severed part correctly only to find that the patient had vomited and aspirated, then asphyxiated while everyone was running about! It reminded me that no matter what horrible development has gone on with a trauma patient's body, none of it matters if you don't have an airway.
So the absolute main point of TNCC and its training is the most basic of principles which hails back to basic life support. A B C!!! Always airway and breathing, even before pulse, since once again, a pulse won't last long if there is no breathing involved.
More nuggets from this wonderful course on another day.
Monday, May 3, 2010
Nurse's Week
Nurse's Week is coming! It is time to reflect on why we became nurses, where we are today, and where we are going. I remember my first nurse's week in 1991 when I was a student at the University of Iowa. I was working as a nurse's assistant and we got a bag with some random goodies inside. I know that I was proud to carry that bag and used it for my lunches.
There is nothing quite like the enthusiasm and bright outlook of a new nurse and I see them enter our emergency department as students and the newly graduated, ready to jump in and save lives. Do those of us who have many years under our belt still go to work with enthusiasm and an excitement about helping others? I would have to say, realistically, a big No. I personally, don't volunteer to take students because I don't feel I'm a very good teacher or have the willingness to talk all day to someone about what I'm doing. I know what I'm doing, I just don't care to explain each step. There are those in our department who routinely get the students or new nurses and I applaud them and will gladly take an extra patient if it means I have no one following me around.
Now yes, I know I was a student and new nurse too. And I remember some unpleasant experiences from nurses who didn't want to take time to teach and even a patient who said to me, after working long hours on her care plan, "I just am not up to a student nurse today". I do remember, after almost 19 years, the faces of the nurses that were kind to me and went out of their way to teach me the ropes. So I know that I am probably missing out on opportunities to influence others by not teaching. In my defense, I did take on an intern last year for 96 hours of mentoring, so I believe I have paid my dues for this first half of my career! And I must say, it was a good experience, I had a great student, and he taught me a thing or two myself! Amazing how new eyes look at an old problem you've struggled with and solved it in minutes! (Cut the back end off of activated charcoal, don't try to squeeze it through the tip!)
Nurses play so many roles and work in all walks of life... schools, jails, community centers, doctors offices, cruise ships, battle fields, helicopters, offices, and hospitals to name a few. It is a noble profession that is one of the most highly regarded in the public eye. The compensation is good even in this struggling economy and job security is almost airtight. As a matter of fact, the worse the economy, the sicker and more stressed the people, and the greater need for our helping hands.
I have wanted to be a nurse since I was 6. I know this because my mother kept an elementary journal and on the first grade page there was a spot for "What I want to be when I grow up". And in my barely legible (still is) handwriting, is "Nurse". I remember the few times I was ever in a hospital - for appendicitis, a fall on my tailbone, and headaches, and I especially recall the emergency nurses and how enthralled I was with them, even in my discomfort. At some later age I do remember thinking that was where I wanted to be. And less than 10 years into my nursing career, I did enter the ER.
I would like to thank all the nurses, from long, long ago, the ones that have passed, and the ones laboring now. It is not a glamorous job by any stretch of the imagination, but it is one that we can feel proud of, and when we someday retire, will no doubt be satisfied with. Mistakes are made, there are times we scowl instead of smile, but there are countless patients out there who I know I've made laugh, comforted, taught, reassured, and whose pain I have fought to relieve. I can't say I look forward to going to work tomorrow, but when I reflect on the past, there's no other job I was meant to do.
There is nothing quite like the enthusiasm and bright outlook of a new nurse and I see them enter our emergency department as students and the newly graduated, ready to jump in and save lives. Do those of us who have many years under our belt still go to work with enthusiasm and an excitement about helping others? I would have to say, realistically, a big No. I personally, don't volunteer to take students because I don't feel I'm a very good teacher or have the willingness to talk all day to someone about what I'm doing. I know what I'm doing, I just don't care to explain each step. There are those in our department who routinely get the students or new nurses and I applaud them and will gladly take an extra patient if it means I have no one following me around.
Now yes, I know I was a student and new nurse too. And I remember some unpleasant experiences from nurses who didn't want to take time to teach and even a patient who said to me, after working long hours on her care plan, "I just am not up to a student nurse today". I do remember, after almost 19 years, the faces of the nurses that were kind to me and went out of their way to teach me the ropes. So I know that I am probably missing out on opportunities to influence others by not teaching. In my defense, I did take on an intern last year for 96 hours of mentoring, so I believe I have paid my dues for this first half of my career! And I must say, it was a good experience, I had a great student, and he taught me a thing or two myself! Amazing how new eyes look at an old problem you've struggled with and solved it in minutes! (Cut the back end off of activated charcoal, don't try to squeeze it through the tip!)
Nurses play so many roles and work in all walks of life... schools, jails, community centers, doctors offices, cruise ships, battle fields, helicopters, offices, and hospitals to name a few. It is a noble profession that is one of the most highly regarded in the public eye. The compensation is good even in this struggling economy and job security is almost airtight. As a matter of fact, the worse the economy, the sicker and more stressed the people, and the greater need for our helping hands.
I have wanted to be a nurse since I was 6. I know this because my mother kept an elementary journal and on the first grade page there was a spot for "What I want to be when I grow up". And in my barely legible (still is) handwriting, is "Nurse". I remember the few times I was ever in a hospital - for appendicitis, a fall on my tailbone, and headaches, and I especially recall the emergency nurses and how enthralled I was with them, even in my discomfort. At some later age I do remember thinking that was where I wanted to be. And less than 10 years into my nursing career, I did enter the ER.
I would like to thank all the nurses, from long, long ago, the ones that have passed, and the ones laboring now. It is not a glamorous job by any stretch of the imagination, but it is one that we can feel proud of, and when we someday retire, will no doubt be satisfied with. Mistakes are made, there are times we scowl instead of smile, but there are countless patients out there who I know I've made laugh, comforted, taught, reassured, and whose pain I have fought to relieve. I can't say I look forward to going to work tomorrow, but when I reflect on the past, there's no other job I was meant to do.
Thursday, April 15, 2010
Overheard In The ED
Everyone hears things from time to time that they just can't believe - inspiring stories, sad stories, tales of great courage... and then there are the things that come out of people's mouth that leave you speechless. I'm sure this happens in every walk of life and line of work, but it is especially prevalent in the emergency department! I often hear co-workers say, "You can't make this stuff up!" or, "Gotta write that one down!" Well I have actually been writing some of them down, though wish I had for the whole 10 years I've been in the department, boy what a book that would be! But I will share some of the nuggets that I have collected!
Today, I went into room 1 to see a patient. The triage sheet states his complaint was "I've been living in my car for 9 months. The policeman put cameras in my feet and I can't work". When asked how he knew they were in his feet he said, "because people know I'm coming before I get there".
Naples has a lot of wealthy and privileged residents. This complaint was overheard in an exam room of a female senior citizen.
"No one pulls up the blankets here!"
From the nurse, "How do you pull up the blankets at home?"
"Well... those are different blankets!"
Should we really be asking our trauma-certified nurses to pull blankets up and fluff pillows? (Most of us actually do, but not because we're asked to!)
We got a patient into room 19 that had altered level of consciousness. His eyes were like bug eyes, very wide but he wasn't saying much. We sat him up to get him undressed and found multiple Fentanyl patches on his back and chest (a narcotic pain medicine delivered in a patch). The nurse who was helping me said, "maybe that's why he's sedated, he's got multiple Fentanyl patches on!". Upon hearing this, the pt. sat straight up, his eyes got wider (if possible) and he said, "Mother of God! Take them off!"
I was working in triage and an older lady was pushing her older mother in a wheelchair into my exam area. She stated "I'm a terrible driver, I got 2 tickets last year. I don't tell them I have no depth perception!" I immediately asked her what kind of car she drove. Look out for a black convertible!
An older, rough-around-the-edges gentleman sat in my triage chair and complained of diarrhea. He told me he had been trying to treat it himself with soda and beer. "The acid and base balance kinda works!"
Again in triage, a man complained of abdominal pain. "The only thing I do wrong is drink rum, smoke cigarettes, and smoke weed." (The only thing?) Then he told me he had also had the plague. When a pulse oximeter was put on his finger he said, "I swear I'm telling the truth!" Apparently he thought it was a lie detector.
And finally, a lady sat down and reported she had a "cold ear" (a cold foot would be an emergency... loss of circulation, but not sure about how you lose circulation to your ear). She then told me about her medical and family history which included a father who had lung cancer in his knees.
Thursday, April 8, 2010
These ER visits may make you cringe -- or laugh By ASSOCIATED PRESS
TAMPA — One woman fell from a galloping horse while texting.
Another woman's bangs caught fire as she peered into a toaster.
More than 818 emergency room trips in the past four years involved "chicken" — dead and alive.
Yes, big recalls of Toyotas or peanut butter may get the headlines, but millions of Americans with oddball injuries fill emergency rooms every year.
Federal regulators review a sample of those visits for signs a product might need to be recalled. Those records provide a view into the dramatic injuries of Americans who seem able to hurt themselves with almost any product made.
Boxes of cereal (cut fingers), cans of pork and beans (falling from a cupboard onto one's head), wood chippers (yes, people stick their hands in) and trombones (more on that below). Hundreds of people suffer piercings gone wrong, thousands fall out of their mobile homes or have objects intractably lodged in orifices.
"Every day, people come in and you just think, 'You gotta be kidding me,'" said Brian Peckler, an ER doctor for 15 years, now at Tampa General. "I mean, what makes a guy think using a fish hook to clean out ear wax is a good idea?"
The tally
Most ER visits are the result of heart attacks, car wrecks and the like. But another wave of patients stumbles into ERs because of careless accidents or failing products.
The U.S. Consumer Product Safety Commission assembles data from about 100 U.S. hospitals to track trends. The safety commission follows up on about 10 percent of the cases or incident reports it receives from hot lines or via e-mail, spokesman Scott Wolfson said.
The several-million record database of this bloody tally breaks down into a few categories: Cell phones, suspicious circumstances, dramatic flair, simply being a guy and Americans' compulsion to demonstrate products, athletic feats or dance moves.
Cell phones
Cell phones receive heaps of blame as states, including Florida, rush to ban texting and driving. But people are finding a wider range of ways to hurt themselves or others with cell phones. Such as:
A 19-year-old male, on the phone while lifting weights, drops a barbell on himself.
A 21-year-old male, riding his bike and texting, crashes, scrapes his face.
A 37-year-old male cutting chicken while on the phone slices his hand.
A 25-year-old male, texting, walks into a telephone pole's guide wire and tells emergency room workers "he might have gotten zapped."
Hundreds of injuries are blamed on the phone in its capacity as a weapon: They're used as missiles or as a bludgeon to beat people on the head.
Suspicious cases
Many of the cases come with a tale, an alibi that suggests more of a back story than patients are willing to admit to the ER staff.
There is the 2006 case of an 18-year-old woman who was "looking for a cell phone in a dumpster at sorority. Had rubber lid of dumpster fall onto head when wind blew." Head injury.
There is the 2004 case of a 24-year-old woman who said she slipped in the shower. Though such accidents are common, she said hers happened when she stepped on a basketball.
Why was the phone in the Dumpster? Why was a basketball in the shower? The records don't reveal.
Federal regulators emphasize that their records are anonymous, contain no geographic data and patients can decline to be interviewed. But some people volunteer their names, which is how they appear in news reports about product recalls.
Dramatic cases
For others, the case record alone provides vivid mental imagery.
Such is the 2006 incident involving a 46-year-old woman: "Husband was wiring Internet when antlers fell off wall and hit patient on top of head." Or the 17-year-old in 2007 who injured himself at band camp while running and playing trombone.
In the dangerous music category, an 11-year-old vigorously playing the violin poked himself in the eyeball with the bow. And proving that Mother was correct — a number of cases involve children running with scissors, almost all resulting in gouged eyeballs.
Peckler, the Tampa doctor, recalls a young man who came to the ER complaining that his girlfriend's iguana bit off his finger — and he had another issue. The grief-stricken girlfriend had given him her antidepressant medication for pain, which metabolized in his body with effects similar to an overdose of Viagra.
Raccoons, possums and snakes seem dangerous, both when attacking people and when people attack them.
Such as the 30-year-old man in 2008, "Chasing a raccoon last night, forgot he had cable set up in yard." Tripped, twisted left wrist. Or the 66-year-old woman who chased a raccoon off her porch, slipped and broke her hip.
About half the raccoon-related incidents involve people slicing their hands while skinning a dead creature. And one 43-year-old man was sleeping on his porch in 2007 when a coon crept in and attacked his ankle.
Being a guy
Men account for 56 percent of the ER visits, according to federal data, though in some areas they dominate the injured.
Men suffer injury in 80 percent of pressure washer cases. Nine in 10 injuries involving "mobile home" and "alcohol" were suffered by men. And 96 percent of "nail gun" cases were men.
"Guys are definitely dumber than women in this regard," Peckler said.
One 37-year-old man tried cutting branches with a circular saw — on top of a running wood chipper. The saw cut off several fingers, which fell into the chipper.
Having a brother appears dangerous as well. Regardless of who was injured, ER records implicate the brother twice as often as the sister.
Demonstrations
"Demonstrate" appears in no small number of cases where less-than-skilled people tried to show off martial arts moves, wedding dances, pogo-stick skills and cheerleader routines.
Though many people consider themselves expert enough to demonstrate something, Robert Cano at University Community Hospital sees scores of cases that prove otherwise.
"Almost nothing good comes after someone says 'Hey, watch this!'" Cano said.
Note the 52-year-old mother, demonstrating judo to her daughter by flipping her husband. Torn left knee.
Other cases: The 25-year-old man demonstrating to children how to climb on monkey bars when his shoulder "snapped." Or the 16-year-old demonstrating a softball technique who stepped on a rake that smacked her in the forehead.
Or the 55-year-old woman showing her grandson how to use a pogo stick — she fell and smacked her head.
Peckler at Tampa General marvels at accidents that should have been fatal but weren't.
His favorite case: the man who was supposed to be watching his 3-year-old, but decided to change his car's oil in the driveway. Seeking a safe holding area, Dad put the child in the car and crawled underneath to drain the oil.
The child knocked the gear shift from park to neutral, and the car's tire rolled over the man's chest.
He suffered no major injuries, Peckler said. But how could anyone survive?
Peckler shrugged and said, "God's strong love for fools."
Another woman's bangs caught fire as she peered into a toaster.
More than 818 emergency room trips in the past four years involved "chicken" — dead and alive.
Yes, big recalls of Toyotas or peanut butter may get the headlines, but millions of Americans with oddball injuries fill emergency rooms every year.
Federal regulators review a sample of those visits for signs a product might need to be recalled. Those records provide a view into the dramatic injuries of Americans who seem able to hurt themselves with almost any product made.
Boxes of cereal (cut fingers), cans of pork and beans (falling from a cupboard onto one's head), wood chippers (yes, people stick their hands in) and trombones (more on that below). Hundreds of people suffer piercings gone wrong, thousands fall out of their mobile homes or have objects intractably lodged in orifices.
"Every day, people come in and you just think, 'You gotta be kidding me,'" said Brian Peckler, an ER doctor for 15 years, now at Tampa General. "I mean, what makes a guy think using a fish hook to clean out ear wax is a good idea?"
The tally
Most ER visits are the result of heart attacks, car wrecks and the like. But another wave of patients stumbles into ERs because of careless accidents or failing products.
The U.S. Consumer Product Safety Commission assembles data from about 100 U.S. hospitals to track trends. The safety commission follows up on about 10 percent of the cases or incident reports it receives from hot lines or via e-mail, spokesman Scott Wolfson said.
The several-million record database of this bloody tally breaks down into a few categories: Cell phones, suspicious circumstances, dramatic flair, simply being a guy and Americans' compulsion to demonstrate products, athletic feats or dance moves.
Cell phones
Cell phones receive heaps of blame as states, including Florida, rush to ban texting and driving. But people are finding a wider range of ways to hurt themselves or others with cell phones. Such as:
A 19-year-old male, on the phone while lifting weights, drops a barbell on himself.
A 21-year-old male, riding his bike and texting, crashes, scrapes his face.
A 37-year-old male cutting chicken while on the phone slices his hand.
A 25-year-old male, texting, walks into a telephone pole's guide wire and tells emergency room workers "he might have gotten zapped."
Hundreds of injuries are blamed on the phone in its capacity as a weapon: They're used as missiles or as a bludgeon to beat people on the head.
Suspicious cases
Many of the cases come with a tale, an alibi that suggests more of a back story than patients are willing to admit to the ER staff.
There is the 2006 case of an 18-year-old woman who was "looking for a cell phone in a dumpster at sorority. Had rubber lid of dumpster fall onto head when wind blew." Head injury.
There is the 2004 case of a 24-year-old woman who said she slipped in the shower. Though such accidents are common, she said hers happened when she stepped on a basketball.
Why was the phone in the Dumpster? Why was a basketball in the shower? The records don't reveal.
Federal regulators emphasize that their records are anonymous, contain no geographic data and patients can decline to be interviewed. But some people volunteer their names, which is how they appear in news reports about product recalls.
Dramatic cases
For others, the case record alone provides vivid mental imagery.
Such is the 2006 incident involving a 46-year-old woman: "Husband was wiring Internet when antlers fell off wall and hit patient on top of head." Or the 17-year-old in 2007 who injured himself at band camp while running and playing trombone.
In the dangerous music category, an 11-year-old vigorously playing the violin poked himself in the eyeball with the bow. And proving that Mother was correct — a number of cases involve children running with scissors, almost all resulting in gouged eyeballs.
Peckler, the Tampa doctor, recalls a young man who came to the ER complaining that his girlfriend's iguana bit off his finger — and he had another issue. The grief-stricken girlfriend had given him her antidepressant medication for pain, which metabolized in his body with effects similar to an overdose of Viagra.
Raccoons, possums and snakes seem dangerous, both when attacking people and when people attack them.
Such as the 30-year-old man in 2008, "Chasing a raccoon last night, forgot he had cable set up in yard." Tripped, twisted left wrist. Or the 66-year-old woman who chased a raccoon off her porch, slipped and broke her hip.
About half the raccoon-related incidents involve people slicing their hands while skinning a dead creature. And one 43-year-old man was sleeping on his porch in 2007 when a coon crept in and attacked his ankle.
Being a guy
Men account for 56 percent of the ER visits, according to federal data, though in some areas they dominate the injured.
Men suffer injury in 80 percent of pressure washer cases. Nine in 10 injuries involving "mobile home" and "alcohol" were suffered by men. And 96 percent of "nail gun" cases were men.
"Guys are definitely dumber than women in this regard," Peckler said.
One 37-year-old man tried cutting branches with a circular saw — on top of a running wood chipper. The saw cut off several fingers, which fell into the chipper.
Having a brother appears dangerous as well. Regardless of who was injured, ER records implicate the brother twice as often as the sister.
Demonstrations
"Demonstrate" appears in no small number of cases where less-than-skilled people tried to show off martial arts moves, wedding dances, pogo-stick skills and cheerleader routines.
Though many people consider themselves expert enough to demonstrate something, Robert Cano at University Community Hospital sees scores of cases that prove otherwise.
"Almost nothing good comes after someone says 'Hey, watch this!'" Cano said.
Note the 52-year-old mother, demonstrating judo to her daughter by flipping her husband. Torn left knee.
Other cases: The 25-year-old man demonstrating to children how to climb on monkey bars when his shoulder "snapped." Or the 16-year-old demonstrating a softball technique who stepped on a rake that smacked her in the forehead.
Or the 55-year-old woman showing her grandson how to use a pogo stick — she fell and smacked her head.
Peckler at Tampa General marvels at accidents that should have been fatal but weren't.
His favorite case: the man who was supposed to be watching his 3-year-old, but decided to change his car's oil in the driveway. Seeking a safe holding area, Dad put the child in the car and crawled underneath to drain the oil.
The child knocked the gear shift from park to neutral, and the car's tire rolled over the man's chest.
He suffered no major injuries, Peckler said. But how could anyone survive?
Peckler shrugged and said, "God's strong love for fools."
Saturday, March 27, 2010
Becoming a Nurse: 5 Things I Wish I Had Known by Lanette Anderson
1. We can’t always help people. I was one of those people who went into nursing for the stereotypical reason of, “I want to help people.” Imagine my surprise when I found out that this isn’t always possible for a variety of reasons. Sometimes no matter what we do, nothing can change an inevitable outcome. Sometimes patients just don’t want our help. We can’t take it personally if that happens. What we can do is always try our best and do what we can to work towards the best outcome possible.
2. The amount of responsibility that we have is incredible. I’ll never forget the first time that I signed my name with “RN” behind it. My first response was “Wow, that looks great!” This was shortly followed by “Wow, I’m the RN and other people are going to come to me and expect me to know the answers, and I’m going to be accountable for the nursing care that these patients receive.” After the terror subsided, I remembered that it was OK that I didn’t know everything, and that the important thing was that I knew when to ask for help.
3. Just because someone has a license to practice nursing doesn’t mean that they can or should. We’ve all worked with someone who fits into this category. Maybe at times we have fit into this category ourselves. It’s a hard thing to admit. One of the great things about nursing is that there are so many options to choose from in terms of practice areas. If one doesn’t suit us, maybe we can find another that does. Sometimes, however, it just isn’t a good career fit or a person isn’t able to safely practice for some reason. Acknowledging it often helps everyone.
4. We don’t need to hear our patients say, “thank you,” to still be committed to doing a good job. I had visions of grateful patients and families giving frequent positive feedback for a job well done. That didn’t happen as often as I had hoped. I came to realize that it wasn’t that important to me. I didn’t need to rely on that to know that I had done my best.
5. Only another nurse can really know what we do every day. When I first became a nurse, I would relate stories about my work to my friends who would look at me with blank stares or the sympathetic, “That must have been tough,” after a bad day. They tried, but nobody could really understand what a “bad day” really meant, except another nurse who had also been there. It made me appreciate my co-workers even more, and recognize that when I needed to de-stress about work, they were my best support group.
Everyone has their own “five things.” Think back; what are yours? Leave a comment and let us know what you wish you had known before you became a nurse.
About the Author: Lanette L. Anderson, MSN, JD, BBA, RN, speaker, writer and educator. Lanette has been in the nursing profession for almost thirty years and has served on a variety of committees with the National Council of State Boards of Nursing and committees for the Council on Licensure, Enforcement, and Regulation. Lanette is passionate about nurse education, and is currently an instructor with two online universities as well as a teacher at the University of Charleston in West Virginia.
Monday, March 1, 2010
Charting tips from a legal point of view
As a legal nurse consultant who spends a lot of time reviewing medical records, I thought I would share a few tips. First of all, the records I review are electronic, they have been scanned into a record-based program. This does not mean that if a hospital doesn't have computer charting, that those records won't become electronic. Many of the pages I review are handwritten. This is a time consuming task!
If you didn't chart it, it wasn't done! That is a common rule of thumb that holds true always. As an RN, you probably monitor your patients well, and it's second nature to know when a particular patient needs closer watching due to their potential to deteriorate. When that patient does "crash" and possibly die, does the record reflect that you were monitoring their vital signs, color, and mental status for the time preceding the event? Or is there a routine assessment done with one set of vital signs and then three hours later, a code blue log. If this patient or his family sues for negligence, the reviewer of the record will be looking for documentation that showed what led up to the event, what the nurse did to intervene, and whether it could have been prevented. Let's face it, it's the nurse, not the doctor who is at the bedside 99.8% of the time!
Make sure you are charting on the right patient! Most of us have computer based charting at the workplace and in order to chart a note, the cursor highlights a patient name and then a record opens where data is to be placed. Very often, you can be looking at a patient's name, but the cursor or highlight is on another patient. We have all done it and doctors do as well, as I have often brought discharge papers to a patient in the ED to find that the name is incorrect and they almost walked out with a prescription they couldn't use! The other side of that story is that another patient now has a discharge diagnosis that makes no sense. While most of us like the checklists, and notations via keyboard instead of handwritten notes and paper charting, the hazards are many.
Document your communications with physicians. Nurses are patient advocates and it is the nurse who will call the MD to get an order for more pain medicine, or to report deteriorating vital signs, or notify him or her of suspicious findings. Does the doctor call back right away? Were orders received and followed through? In the ED, it is relatively easy since the physician is in the department, but notes should still reflect who was talked to, and if new orders were received. This includes not getting an order. When you tell a physician that the patient is having increased chest pain and he declines a response, if the patient arrests, your documentation could help you defend your actions if there happens to be a suit. A nurse who works on a floor and has to call a physician should document as well. How long was the response time? Were you ignored or did you get appropriate orders?
If you go back and add an entry because you didn't have time or you remembered something later, chart it as "late entry" with the date and time. With most computer charting, times can be altered electronically, but you want to make sure that your entries don't look suspicious or suggest tampering.
Get credit for all you do! Nurses routinely put up side rails, leave call lights, and monitor safety. Some records have a check-mark system to note that these things have been done. If not, write it yourself. If your patient falls out of bed and breaks a hip, can the family go to court and say the nurse left the side-rails down and a confused patient unattended? Of course medication administration is a big focus for hospitals. Medication errors injure millions of people and cost billions of dollars annually. Many hospitals have bar codes that must be scanned or other methods to confirm that you are administering to the correct patient. But do you have the correct pill? Is it the right time? And if you are giving Digoxin, did you note that the patient's heart rate is above 60? A nurse cannot double check enough when it comes to this critical role of dispensing medications.
Some No-No's:
Don't chart a symptom without noting what you did about it. If you write that the patient's nose began bleeding, does the chart reflect what you did? Who you notified? Did you give a dose of Plavix or Coumadin two hours later?
Do not alter a patient's record - in regards to a paper chart. Blacking out an entry or going back to change something after the fact is a criminal offense.
Don't use imprecise descriptions. "Patient in a lot of pain". Document that chest pain is 8/10. "The incision is wide open". Chart that the incision is 1.5 cm wide, 3 cm long and unapproximated.
Don't chart something you haven't done or something you plan to do. It may seem obvious, but you may not do something you plan to and charting care you haven't done is fraud.
Don't chart unaccepted abbreviations. Check with your institution, most have a list of accepted abbreviations. Our facility allows a nurse to chart "Patient is alert, NAD". This is known to most as "no apparent distress". On the other hand, our facility does not allow us to chart "Aspirin QD". We must write "daily". Abbreviations with medications are tricky because a wrong abbreviation when taking verbal orders can cause a patient to be administered medications incorrectly. Will that MD defend himself as having given a correct verbal order if he is taken to court? Absolutely, the nurse who wrote the order is on her own.
Charting is a part of every nurse's life and shouldn't be a cause for anxiety. It should be looked at as your proof that you have performed your duties well and as competently as the next nurse, if not more so. Leave at the end of a shift knowing that you have safeguarded your professional future and will be ready to start the process over tomorrow.
If you didn't chart it, it wasn't done! That is a common rule of thumb that holds true always. As an RN, you probably monitor your patients well, and it's second nature to know when a particular patient needs closer watching due to their potential to deteriorate. When that patient does "crash" and possibly die, does the record reflect that you were monitoring their vital signs, color, and mental status for the time preceding the event? Or is there a routine assessment done with one set of vital signs and then three hours later, a code blue log. If this patient or his family sues for negligence, the reviewer of the record will be looking for documentation that showed what led up to the event, what the nurse did to intervene, and whether it could have been prevented. Let's face it, it's the nurse, not the doctor who is at the bedside 99.8% of the time!
Make sure you are charting on the right patient! Most of us have computer based charting at the workplace and in order to chart a note, the cursor highlights a patient name and then a record opens where data is to be placed. Very often, you can be looking at a patient's name, but the cursor or highlight is on another patient. We have all done it and doctors do as well, as I have often brought discharge papers to a patient in the ED to find that the name is incorrect and they almost walked out with a prescription they couldn't use! The other side of that story is that another patient now has a discharge diagnosis that makes no sense. While most of us like the checklists, and notations via keyboard instead of handwritten notes and paper charting, the hazards are many.
Document your communications with physicians. Nurses are patient advocates and it is the nurse who will call the MD to get an order for more pain medicine, or to report deteriorating vital signs, or notify him or her of suspicious findings. Does the doctor call back right away? Were orders received and followed through? In the ED, it is relatively easy since the physician is in the department, but notes should still reflect who was talked to, and if new orders were received. This includes not getting an order. When you tell a physician that the patient is having increased chest pain and he declines a response, if the patient arrests, your documentation could help you defend your actions if there happens to be a suit. A nurse who works on a floor and has to call a physician should document as well. How long was the response time? Were you ignored or did you get appropriate orders?
If you go back and add an entry because you didn't have time or you remembered something later, chart it as "late entry" with the date and time. With most computer charting, times can be altered electronically, but you want to make sure that your entries don't look suspicious or suggest tampering.
Get credit for all you do! Nurses routinely put up side rails, leave call lights, and monitor safety. Some records have a check-mark system to note that these things have been done. If not, write it yourself. If your patient falls out of bed and breaks a hip, can the family go to court and say the nurse left the side-rails down and a confused patient unattended? Of course medication administration is a big focus for hospitals. Medication errors injure millions of people and cost billions of dollars annually. Many hospitals have bar codes that must be scanned or other methods to confirm that you are administering to the correct patient. But do you have the correct pill? Is it the right time? And if you are giving Digoxin, did you note that the patient's heart rate is above 60? A nurse cannot double check enough when it comes to this critical role of dispensing medications.
Some No-No's:
Don't chart a symptom without noting what you did about it. If you write that the patient's nose began bleeding, does the chart reflect what you did? Who you notified? Did you give a dose of Plavix or Coumadin two hours later?
Do not alter a patient's record - in regards to a paper chart. Blacking out an entry or going back to change something after the fact is a criminal offense.
Don't use imprecise descriptions. "Patient in a lot of pain". Document that chest pain is 8/10. "The incision is wide open". Chart that the incision is 1.5 cm wide, 3 cm long and unapproximated.
Don't chart something you haven't done or something you plan to do. It may seem obvious, but you may not do something you plan to and charting care you haven't done is fraud.
Don't chart unaccepted abbreviations. Check with your institution, most have a list of accepted abbreviations. Our facility allows a nurse to chart "Patient is alert, NAD". This is known to most as "no apparent distress". On the other hand, our facility does not allow us to chart "Aspirin QD". We must write "daily". Abbreviations with medications are tricky because a wrong abbreviation when taking verbal orders can cause a patient to be administered medications incorrectly. Will that MD defend himself as having given a correct verbal order if he is taken to court? Absolutely, the nurse who wrote the order is on her own.
Charting is a part of every nurse's life and shouldn't be a cause for anxiety. It should be looked at as your proof that you have performed your duties well and as competently as the next nurse, if not more so. Leave at the end of a shift knowing that you have safeguarded your professional future and will be ready to start the process over tomorrow.
Friday, February 26, 2010
Take your cholesterol medicine at night!
"Statins" are the most prescribed cholesterol medicine. They lower LDL levels - the "bad cholesterol" and the reduction of the total cholesterol results in large reductions in heart attacks and complications from heart disease. Statins inhibit the enzyme HMG-CoA reductase that is in charge of the rate of cholesterol production in the body. The medicine slows down the production of cholesterol and helps the liver remove the LDL cholesterol already in the blood.
Most people like to simplify life and take all their medicines at one time. But there are reasons for taking medicine at other times. The body makes more cholesterol at night and when the statin is taken just before bedtime, it is more potent in your body. So if you are going to commit to taking the drug, let it do the most for you!
Most people like to simplify life and take all their medicines at one time. But there are reasons for taking medicine at other times. The body makes more cholesterol at night and when the statin is taken just before bedtime, it is more potent in your body. So if you are going to commit to taking the drug, let it do the most for you!
Sunday, February 21, 2010
Interview with Vickie L. Milazzo, legal nurse consultant
How did you go from nurse to legal nurse consultant?
Even when I was in nursing school, I knew I was interested in owning a business. I explored different options. One area I was interested in was patient education, and I did some classes for health care consumers. But the system didn't really offer the opportunity to make a business out of it. The income opportunities would not allow me to give up my day job.
Then, in 1981, a friend who was a psychiatric nurse was involved in a legal case as an expert witness to an attorney. When she told me about it, the lightbulb just went off and I said, "I know I can do that." When I was little, I wanted to be a lot of things. One of the things I had on my list was attorney.
How did you get your first case?
Back then, RNs sometimes were hired as expert witnesses, but none with a full-time career as a legal nurse consultant. I still worked in the hospital and I marketed myself to attorneys, trying to educate them about what I could do for them as a nurse.
I asked a woman who had done typing for me if she knew any RNs who worked for attorneys. She knew a nurse who did life care planning and this nurse put me in touch with an attorney. He said he was engaged with a case and told me to call him back. I called him back three times before he was able to talk to me.
When I started to work for him, he requested that I only research articles and literature. I was excited at the idea of earning $40 an hour to do that, but I thought, "How's he to know what an RN can do for him?" So I researched the articles and wrote a five-page opinion report. He said, "This report is going to help me more than this stack of articles. Here's a second case, write me a report." In the beginning, I educated the attorneys and they educated me.
What has been your most interesting case?
I always go back to the Genene Jones case. [Jones, an LVN who worked at hospitals in the Austin area, was convicted in 1984 for the murder of two children and is suspected of murdering at least 20 other babies in her care.] It was a civil case filed by the parents of a young child who was allegedly killed by Jones.
The child had accompanied her sister to the pediatrician's office. Jones allegedly grabbed her and said, "This child is due for a vaccination," and injected her with Anectine (succinylcholine chloride). After the injection, the child arrested and died. At first, I was a little bit in disbelief when the attorney hired me. It was hard for me to believe that a nurse would commit that kind of act. Ultimately, it was painful to me as an RN when it became clear that the plaintiff's allegations were valid.
What was your role in the case?
I went through the medical records. I especially tried to show how Jones' documentation was not consistent with standard documentation done by RNs. Her documentation was quite bizarre. I also reviewed peer committee reports. The case was eventually settled out of court.
What does a nurse legal consultant do?
There are about 30 different things that legal nurse consultants do for lawyers. We help them analyze the case. We transcribe medical records, screen the cases for merit, locate expert witnesses and write reports as study aids for the attorney. We write 25- or 50-page reports, whereas an expert witness might write only one or two pages. We also help with the discovery process.
How much does a legal nurse
consultant earn?
Some nurses work in-house and some are independent consultants with their own businesses. An independent consultant might make between $75 and $100 an hour, while a nurse who works in-house might earn $20 an hour.
What do you teach in your classes?
We teach everything from the role of the legal nurse consultant to legal theories and how to apply them as a legal nurse consultant. We teach the litigation process. We teach how to screen and how to write reports. We hold an intensive six-day program. We also have a whole day on marketing and business development because nurses tend to not have those skills.
Last year, I trained about 2,000 nurses. In all, I've probably trained 15,000 to 20,000 nurses.
Why did you become a nurse?
When I was a senior in high school, my father had a cardiac bypass. I was impressed with the role of the nurses who cared for my father. Also, I had worked as a candy striper in high school and my sister was an RN. My mother had always wanted to be a nurse. Really, I wanted to be a lot of things. I wanted to be a doctor, I wanted to be an attorney, I wanted to be a journalist. But that was the era when young girls weren't encouraged to do those things. Our choices were nursing and teaching.
It's interesting because now, later in life, my interests have merged. I write. I teach. I get to do the things in the two areas I love-health care and the law. I'm able to help nurses who want to change their careers.
I miss healing patients, but I get to do that with RNs now. I still think of myself as a healer, but I think we can nurture and heal all kinds of people.
Even when I was in nursing school, I knew I was interested in owning a business. I explored different options. One area I was interested in was patient education, and I did some classes for health care consumers. But the system didn't really offer the opportunity to make a business out of it. The income opportunities would not allow me to give up my day job.
Then, in 1981, a friend who was a psychiatric nurse was involved in a legal case as an expert witness to an attorney. When she told me about it, the lightbulb just went off and I said, "I know I can do that." When I was little, I wanted to be a lot of things. One of the things I had on my list was attorney.
How did you get your first case?
Back then, RNs sometimes were hired as expert witnesses, but none with a full-time career as a legal nurse consultant. I still worked in the hospital and I marketed myself to attorneys, trying to educate them about what I could do for them as a nurse.
I asked a woman who had done typing for me if she knew any RNs who worked for attorneys. She knew a nurse who did life care planning and this nurse put me in touch with an attorney. He said he was engaged with a case and told me to call him back. I called him back three times before he was able to talk to me.
When I started to work for him, he requested that I only research articles and literature. I was excited at the idea of earning $40 an hour to do that, but I thought, "How's he to know what an RN can do for him?" So I researched the articles and wrote a five-page opinion report. He said, "This report is going to help me more than this stack of articles. Here's a second case, write me a report." In the beginning, I educated the attorneys and they educated me.
What has been your most interesting case?
I always go back to the Genene Jones case. [Jones, an LVN who worked at hospitals in the Austin area, was convicted in 1984 for the murder of two children and is suspected of murdering at least 20 other babies in her care.] It was a civil case filed by the parents of a young child who was allegedly killed by Jones.
The child had accompanied her sister to the pediatrician's office. Jones allegedly grabbed her and said, "This child is due for a vaccination," and injected her with Anectine (succinylcholine chloride). After the injection, the child arrested and died. At first, I was a little bit in disbelief when the attorney hired me. It was hard for me to believe that a nurse would commit that kind of act. Ultimately, it was painful to me as an RN when it became clear that the plaintiff's allegations were valid.
What was your role in the case?
I went through the medical records. I especially tried to show how Jones' documentation was not consistent with standard documentation done by RNs. Her documentation was quite bizarre. I also reviewed peer committee reports. The case was eventually settled out of court.
What does a nurse legal consultant do?
There are about 30 different things that legal nurse consultants do for lawyers. We help them analyze the case. We transcribe medical records, screen the cases for merit, locate expert witnesses and write reports as study aids for the attorney. We write 25- or 50-page reports, whereas an expert witness might write only one or two pages. We also help with the discovery process.
How much does a legal nurse
consultant earn?
Some nurses work in-house and some are independent consultants with their own businesses. An independent consultant might make between $75 and $100 an hour, while a nurse who works in-house might earn $20 an hour.
What do you teach in your classes?
We teach everything from the role of the legal nurse consultant to legal theories and how to apply them as a legal nurse consultant. We teach the litigation process. We teach how to screen and how to write reports. We hold an intensive six-day program. We also have a whole day on marketing and business development because nurses tend to not have those skills.
Last year, I trained about 2,000 nurses. In all, I've probably trained 15,000 to 20,000 nurses.
Why did you become a nurse?
When I was a senior in high school, my father had a cardiac bypass. I was impressed with the role of the nurses who cared for my father. Also, I had worked as a candy striper in high school and my sister was an RN. My mother had always wanted to be a nurse. Really, I wanted to be a lot of things. I wanted to be a doctor, I wanted to be an attorney, I wanted to be a journalist. But that was the era when young girls weren't encouraged to do those things. Our choices were nursing and teaching.
It's interesting because now, later in life, my interests have merged. I write. I teach. I get to do the things in the two areas I love-health care and the law. I'm able to help nurses who want to change their careers.
I miss healing patients, but I get to do that with RNs now. I still think of myself as a healer, but I think we can nurture and heal all kinds of people.
Monday, February 15, 2010
My Introduction
I am starting my blog with an eye on the future but my mind filled with experiences of my past. I'm sure I am like many... I have a lot to share but stumble to get the controls to the right vehicle.
So, let's try a blog! Informal, yet professional looking. Economical (ie: free) and easy to use yet with the ability to reach the millions of eyes out there cruising the internet. What do I want to get out there?
Ahh... that is what it's all about!
My name is a start. It is Emily Goggin. Born as Emily Borneman, married as Emily Flynn and remarried as Emily Goggin. The last time - and I do mean last time - I debated changing my name because I had worked many years as a professional with the last name Flynn and shared the name with my 2 boys. But I am wholly committed to my husband and our future, so gladly changed my name and this is where it will stay until it adorns a shiny marble stone far in the future.
I am an only child and my mom kept a detailed school scrapbook. On my first grade page it asked what I want to be. "Nurse" is scribbled in the blank and a nurse is what I became. I grew up in a Chicago suburb but went to the University of Iowa for my training - a truly great school. I wrote my boards and got my first job in Naples, Florida, following my fiance and his family to the sunny state.
I started at Naples Community Hospital (NCH) on a medical-surgical floor, quickly got accepted into a critical care internship, and landed a night shift in a progressive care unit. My first son was born a few years later and I followed a friend into home health care and spent a great 4 years working for a terrific agency which has since dissolved. The co-workers and friends from that job are with me still. I returned to NCH to a telemetry floor, and after a few years, in 2000 started in the emergency department. I have left briefly for a cardiology office job and home health intake coordinator job while I tried to navigate parenting 2 small boys and 12 hour shifts, but the ER is where I am to stay.
Somewhere in there I studied a home course and took an exam to become a Certified Legal Nurse Consultant because I'm always looking for more - more experiences, more money, better hours. And this field offered it all! But beware, you don't put down the pen from the exam and start billing $100 an hour! There is this little thing called marketing which I think should be a 4 letter word! I did what I was told to do in the course (though I don't know how well) and got no where. I did start a website and paid to list myself on a page of experts and did eventually get some work. One of the parties that contacted me is a story unto itself - for another time. But I got some experience reviewing cases both for the plaintiff and the defense and was deposed one time. I collected my fees and then let my marketing lapse. I figured it wasn't for me.
I have always kept my eye on a Yahoo group listserve and saw a posting for a group looking for nurses to review records at home. I contacted them and before I knew it, was on a conference training call and then working from my home for an hourly rate, the same as that at the hospital. It wasn't big bucks, but it was constant work and no 45 minute commute. I have been working on a class action suit since last April and have learned a lot. We were on hold for 2 months before Christmas while the company debated if they would continue litigation, so I also learned to not quit your day job!
That brings me to the present! I still want more! I'm working 50 hours a week - 24 at the hospital, 30 at home. But being at home, it doesn't feel like I'm putting in such serious hours. I would like to get myself back out there and market myself for other consulting work. I have admired other nurse's websites - hospital nurses and legal nurses, and want to start my own.
So here I go. Bear with me and I'll try to make it interesting and fun. Because ultimately, I want to have fun... get up late... have a maid... a summer home... and travel to Italy, Greece, and Egypt. So I have lot of work to do!
So, let's try a blog! Informal, yet professional looking. Economical (ie: free) and easy to use yet with the ability to reach the millions of eyes out there cruising the internet. What do I want to get out there?
Ahh... that is what it's all about!
My name is a start. It is Emily Goggin. Born as Emily Borneman, married as Emily Flynn and remarried as Emily Goggin. The last time - and I do mean last time - I debated changing my name because I had worked many years as a professional with the last name Flynn and shared the name with my 2 boys. But I am wholly committed to my husband and our future, so gladly changed my name and this is where it will stay until it adorns a shiny marble stone far in the future.
I am an only child and my mom kept a detailed school scrapbook. On my first grade page it asked what I want to be. "Nurse" is scribbled in the blank and a nurse is what I became. I grew up in a Chicago suburb but went to the University of Iowa for my training - a truly great school. I wrote my boards and got my first job in Naples, Florida, following my fiance and his family to the sunny state.
I started at Naples Community Hospital (NCH) on a medical-surgical floor, quickly got accepted into a critical care internship, and landed a night shift in a progressive care unit. My first son was born a few years later and I followed a friend into home health care and spent a great 4 years working for a terrific agency which has since dissolved. The co-workers and friends from that job are with me still. I returned to NCH to a telemetry floor, and after a few years, in 2000 started in the emergency department. I have left briefly for a cardiology office job and home health intake coordinator job while I tried to navigate parenting 2 small boys and 12 hour shifts, but the ER is where I am to stay.
Somewhere in there I studied a home course and took an exam to become a Certified Legal Nurse Consultant because I'm always looking for more - more experiences, more money, better hours. And this field offered it all! But beware, you don't put down the pen from the exam and start billing $100 an hour! There is this little thing called marketing which I think should be a 4 letter word! I did what I was told to do in the course (though I don't know how well) and got no where. I did start a website and paid to list myself on a page of experts and did eventually get some work. One of the parties that contacted me is a story unto itself - for another time. But I got some experience reviewing cases both for the plaintiff and the defense and was deposed one time. I collected my fees and then let my marketing lapse. I figured it wasn't for me.
I have always kept my eye on a Yahoo group listserve and saw a posting for a group looking for nurses to review records at home. I contacted them and before I knew it, was on a conference training call and then working from my home for an hourly rate, the same as that at the hospital. It wasn't big bucks, but it was constant work and no 45 minute commute. I have been working on a class action suit since last April and have learned a lot. We were on hold for 2 months before Christmas while the company debated if they would continue litigation, so I also learned to not quit your day job!
That brings me to the present! I still want more! I'm working 50 hours a week - 24 at the hospital, 30 at home. But being at home, it doesn't feel like I'm putting in such serious hours. I would like to get myself back out there and market myself for other consulting work. I have admired other nurse's websites - hospital nurses and legal nurses, and want to start my own.
So here I go. Bear with me and I'll try to make it interesting and fun. Because ultimately, I want to have fun... get up late... have a maid... a summer home... and travel to Italy, Greece, and Egypt. So I have lot of work to do!
Subscribe to:
Comments (Atom)