
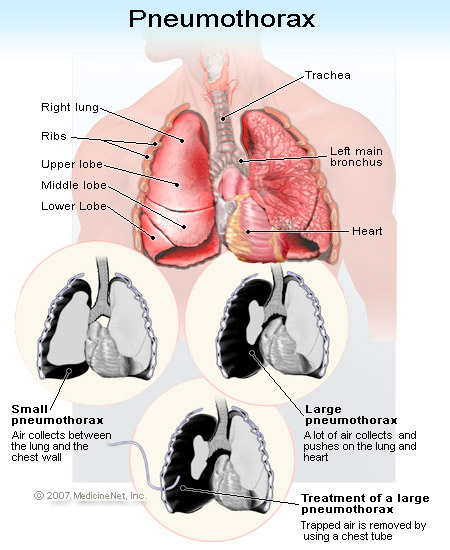
So what is a pneumothorax? A pneumothorax is a collection of free air in the chest outside the lung that causes the lung to collapse. A spontaneous pneumothorax, also referred to as a primary pneumothorax, occurs in the absence of a traumatic injury to the chest or a known lung disease. It is caused by a rupture of a cyst or a small sac (bleb) on the surface of the lung. Pneumothorax may also occur following an injury to the chest wall such as a fractured rib, any penetrating injury (gun shot or stabbing), surgical invasion of the chest, or may be deliberately induced in order to collapse the lung. A pneumothorax can also develop as a result of underlying lung diseases, including cystic fibrosis, chronic obstructive pulmonary disease (COPD), lung cancer, asthma, and infections of the lungs.
Spontaneous pneumothorax affects about 9,000 persons each year in the U.S. who have no history of lung disease. Smoking has been shown to increase the risk for spontaneous pneumothorax.
To verify diagnosis, examination of the chest with a stethoscope reveals decreased or absent breath sounds over the affected lung. The diagnosis is confirmed by chest x-ray.
A small pneumothorax without underlying lung disease may resolve on its own in one to two weeks. A larger pneumothorax and a pneumothorax associated with underlying lung disease often require aspiration of the free air and/or placement of a chest tube to evacuate the air. Possible complications of chest tube insertion include pain, infection of the space between the lung and chest wall (the pleural space), hemorrhage (bleeding), fluid accumulation in the lung, and low blood pressure (hypotension). In some cases, the leak does not close on its own. This is called a bronchopleural fistula, and may require chest surgery to repair the hole in the lung.
The outcome of a pneumothorax depends upon the extent and type of pneumothorax. A small spontaneous pneumothorax will generally resolve on its own without treatment. A secondary pneumothorax associated with underlying disease, even when small, is much more serious and carries a 15% mortality rate. A secondary pneumothorax requires urgent and immediate treatment. Having one pneumothorax increases the risk of developing the condition again. The recurrence rate for both primary and secondary pneumothorax is about 40%; most recurrences occur within 1.5 to two years.
The nurse’s role in the ED is vital in identification upon presentation and in carrying out treatment. The patient will be understandably anxious, scared and uncomfortable. Education and reassurance needs to be given to both the patient and family members. The ED physician will need assistance if a chest tube is to be inserted and preparation includes obtaining consent, set up of the equipment, and pre-medications and monitoring of vital signs/oxygenation. The patient will most times be admitted and will need follow up care. Try to bite your tongue on the smoking cessation lecture (if warranted) until the patient is once again comfortable!
Medical Revising Authors and Editor: George Schiffman, MD, and Melissa Conrad Stoppler, MD
No comments:
Post a Comment